Clinical document confidentiality rules: 2026 guide
Clinical document confidentiality rules are the legal and operational standards that govern how healthcare organisations collect, store, use, and disclose sensitive patient information. In the United States, these rules are anchored primarily in the HIPAA Privacy Rule, the HIPAA Security Rule, and 42 CFR Part 2, each addressing distinct categories of protected health information (PHI). For healthcare professionals, legal experts, and compliance officers, understanding where these frameworks overlap and where they diverge is not optional. A single misstep in handling confidentiality in medical records can trigger federal penalties, erode patient trust, and expose organisations to civil litigation.
What are the core federal regulations governing clinical document confidentiality?
The HIPAA Privacy Rule defines PHI as any individually identifiable health information held or transmitted by a covered entity or its business associates, regardless of format. It grants patients the right to access, amend, and request restrictions on their records. It also limits permissible disclosures to treatment, payment, and healthcare operations without requiring patient authorisation.
The HIPAA Security Rule narrows its focus to electronic PHI (e-PHI). It mandates administrative, physical, and technical safeguards to protect e-PHI from unauthorised access, alteration, or destruction. Risk analysis is not a one-time exercise under this rule. Covered entities must conduct ongoing assessments and update their controls as systems and threats evolve.

42 CFR Part 2 operates alongside HIPAA but applies specifically to records from federally assisted substance use disorder (SUD) treatment programmes. Its restrictions are considerably stricter. Where HIPAA permits disclosure for treatment coordination without consent, Part 2 generally prohibits identifying a person as having or having had a SUD without written consent or a qualifying court order.
The 2026 Part 2 final rule introduces a significant alignment with HIPAA by permitting a single consent for future uses and redisclosure by HIPAA-covered entities, subject to conditions. This reduces administrative burden while preserving the rule’s core protections for legal proceedings. Compliance officers should treat this update as a trigger to audit existing consent workflows immediately.
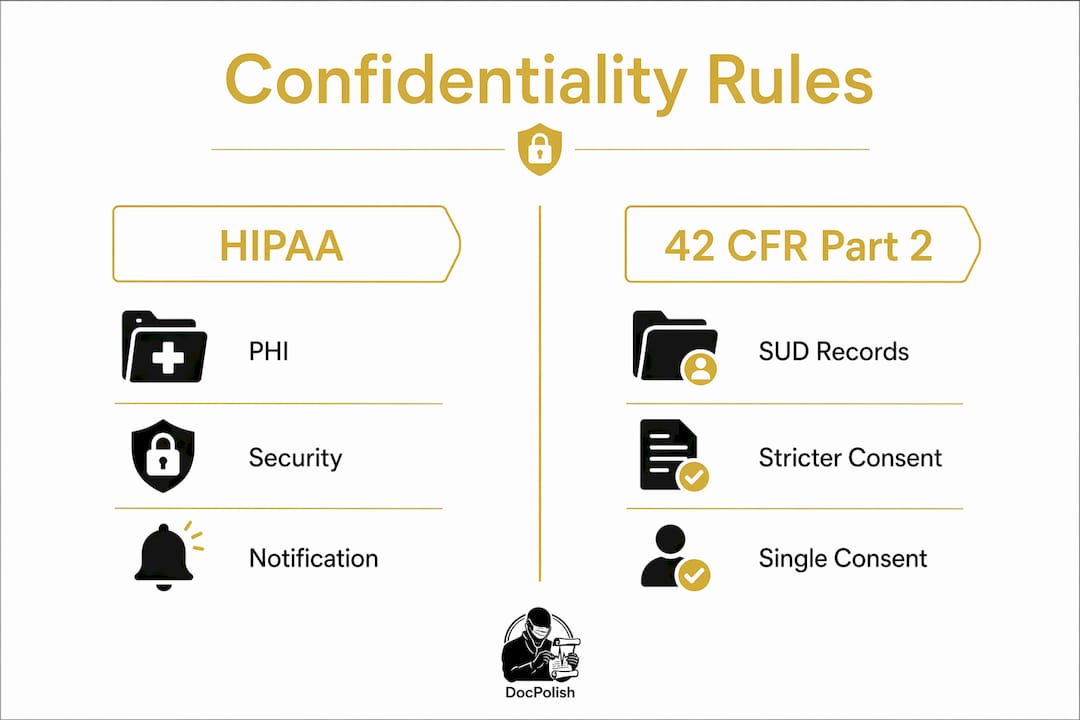
Key distinctions between HIPAA and Part 2 at a glance:
- HIPAA covers all PHI held by covered entities and business associates across all conditions and treatments.
- 42 CFR Part 2 applies exclusively to records from federally assisted SUD programmes, with stricter consent and legal-use restrictions.
- Overlap occurs when a HIPAA-covered entity also operates a Part 2 programme, requiring parallel compliance frameworks.
- Disclosure for legal proceedings is broadly permitted under HIPAA with appropriate authorisation, but is highly restricted under Part 2 regardless of consent.
Pro Tip: When your organisation operates both general clinical services and a federally assisted SUD programme, map each document type to its governing framework before building any disclosure workflow. Treating all records as standard PHI is one of the most common and costly compliance errors in mixed-service settings.
How do clinical document confidentiality rules differ for SUD records?
The elevated protections under 42 CFR Part 2 reflect a deliberate policy choice. Congress recognised that the stigma attached to substance use disorders creates a unique deterrent effect. If patients fear their treatment records could be used against them in court or shared with employers, they will avoid seeking care. The law therefore builds in protections that go well beyond standard patient data privacy laws.
Part 2 covers any programme that holds itself out as providing SUD diagnosis, treatment, or referral, and that receives federal assistance in any form, including Medicare or Medicaid reimbursement. The practical scope is broad. Most hospital-based addiction medicine units, outpatient SUD clinics, and opioid treatment programmes fall within its reach.
The consent requirements under Part 2 are specific and non-negotiable:
- Written consent must name the specific person or organisation authorised to make the disclosure.
- The consent must identify the specific individual or entity to whom disclosure is made.
- It must state the purpose of the disclosure.
- It must include an expiry date or condition.
- It must inform the patient of their right to revoke consent at any time.
The 2026 single-consent provision now allows a patient to sign one consent form covering future uses and redisclosures by HIPAA-covered entities for treatment, payment, and operations. This is a meaningful operational improvement, but it does not extend to legal proceedings. SUD records remain prohibited from use in civil, criminal, administrative, or legislative proceedings against a patient without specific consent or a qualifying court order.
Pro Tip: Train your clinical and billing staff separately on Part 2 workflows. Billing teams accustomed to routine HIPAA-permitted disclosures will inadvertently violate Part 2 if they apply the same logic to SUD records. A short, scenario-based training module specific to Part 2 consent requirements pays for itself after the first avoided penalty.
The operational impact is real. Organisations must maintain separate document-handling queues, apply document-type tagging to distinguish Part 2 records from standard PHI, and build consent-verification checkpoints into every disclosure pathway. Knowing what counts as patient PII across these overlapping frameworks is the starting point for any compliant workflow design.
What are the HIPAA breach notification requirements for clinical documents?
A breach under HIPAA is defined as the acquisition, access, use, or disclosure of unsecured PHI in a manner not permitted by the Privacy Rule. The definition covers both electronic and physical records. A misfiled paper chart and an unencrypted email containing patient data are both potential breaches.
The HIPAA Breach Notification Rule requires covered entities to notify affected individuals, the HHS Office for Civil Rights (OCR), and, where the breach affects more than 500 residents of a state or jurisdiction, the relevant media outlets. All notifications must be issued within 60 days of discovering the breach. This deadline is firm. Organisations that delay notification while conducting internal investigations routinely find themselves in double jeopardy, facing both the original breach and a notification violation.
Notification content must include:
- A description of what happened, including the date of the breach and the date of discovery.
- The types of PHI involved, such as names, dates of birth, diagnosis codes, or financial information.
- Steps individuals should take to protect themselves from potential harm.
- A brief description of what the covered entity is doing to investigate, mitigate harm, and prevent future breaches.
- Contact details for individuals to ask questions or obtain further information.
Risk assessment is the gateway to determining whether notification is required at all. Covered entities must evaluate four factors: the nature and extent of the PHI involved, who accessed or could have accessed it, whether the PHI was actually acquired or viewed, and the extent to which the risk has been mitigated. If this assessment demonstrates a low probability that PHI was compromised, notification may not be required. Documenting that assessment thoroughly is as important as the assessment itself.
For organisations handling sensitive data across clinical and legal workflows, guidance on handling sensitive data documents securely provides a practical framework for reducing breach exposure at the document level.
How should healthcare entities implement effective confidentiality controls?
Effective patient information safeguarding requires controls across three domains defined by the HIPAA Security Rule: administrative, physical, and technical. Treating these as a checklist rather than an integrated programme is where most compliance failures originate.
| Control domain | Standard PHI requirements | Part 2 SUD record requirements |
|---|---|---|
| Administrative | Privacy policies, workforce training, access management | Separate consent workflows, staff training specific to Part 2, designated Part 2 compliance lead |
| Physical | Locked storage, visitor access logs, workstation controls | Segregated physical filing, restricted access to SUD programme areas |
| Technical | Encryption, audit logs, user authentication | Document-type tagging, consent-verification checkpoints, redisclosure controls |
Administrative safeguards form the foundation. Organisations must designate a privacy officer, implement written privacy and security policies, train all workforce members with access to PHI, and establish sanctions for policy violations. These are not aspirational standards. The OCR expects documented evidence of each element during an audit.
Physical safeguards address the environment in which PHI is stored and accessed. Workstation use policies, facility access controls, and device and media disposal procedures all fall within this category. For SUD records, physical segregation of paper files and restricted access to electronic record systems housing Part 2 data add an additional layer of protection.
Technical safeguards are where compliance programmes must integrate privacy policies with security controls. Encryption of e-PHI at rest and in transit, unique user identification, automatic logoff, and audit controls are the core requirements. The 2026 CMS final rule adds a further dimension by mandating secure electronic signatures and authenticated document exchange for health care claims attachments. This affects how clinical documentation moves through billing and claims workflows, and compliance officers should verify that their claims systems meet the new authentication standards.
Document-type tagging deserves particular attention. Organisations handling mixed clinical document sets must implement tagging systems that flag Part 2 records at the point of creation, triggering the appropriate consent-verification and disclosure-restriction workflows automatically. Manual identification is unreliable at scale. Integrating tagging into the electronic health record (EHR) system at the template level is the most dependable approach. For teams managing document editing and review, keeping confidential client data safe during those processes is a compliance obligation, not merely a best practice.
Pro Tip: Run a tabletop exercise annually that simulates a Part 2 redisclosure request arriving through your standard HIPAA disclosure pathway. The exercise will expose gaps in your tagging and routing systems faster than any policy review.
Key takeaways
Clinical document confidentiality rules require organisations to operate parallel compliance frameworks under HIPAA and 42 CFR Part 2, with distinct consent, disclosure, and safeguard obligations for each.
| Point | Details |
|---|---|
| HIPAA and Part 2 are not interchangeable | Part 2 imposes stricter consent and legal-use restrictions than HIPAA for SUD treatment records. |
| 2026 Part 2 single consent | The new single-consent provision reduces administrative burden but does not extend to legal proceedings. |
| Breach notification deadline | Covered entities must notify individuals and HHS OCR within 60 days of discovering a breach. |
| Document-type tagging is non-negotiable | Tagging Part 2 records at creation prevents inadvertent HIPAA-standard disclosures of SUD data. |
| Technical safeguards must meet 2026 CMS standards | Claims attachment workflows now require secure electronic signatures and authenticated document exchange. |
Where compliance teams consistently underestimate the complexity
Working alongside compliance officers in mixed-service healthcare settings, the pattern I see most often is not wilful non-compliance. It is structural underestimation. Teams build one privacy framework, label it HIPAA-compliant, and assume it covers everything. It does not. The moment a federally assisted SUD programme is in the mix, that single framework becomes legally insufficient for a significant subset of records.
The 2026 Part 2 updates are genuinely helpful. Single consent for treatment, payment, and operations disclosures removes a real administrative burden. But I have watched compliance teams treat the update as a simplification of Part 2 overall, when in fact the legal-proceedings prohibition remains as strict as ever. That misreading creates exactly the kind of gap that surfaces during an OCR investigation.
The other underestimated area is the Notice of Privacy Practices. HIPAA requires entities to disclose when more stringent laws apply than HIPAA itself, including Part 2. Most NPPs I have reviewed either omit this entirely or bury it in language patients cannot parse. Patient-centred communication about confidentiality rights is not a regulatory formality. It is the mechanism by which patients make informed decisions about their care. Organisations that treat it as a box-ticking exercise are one complaint away from an OCR investigation.
The practical remediation is straightforward: audit your NPP annually, map every document type to its governing framework, and test your disclosure workflows with realistic scenarios rather than theoretical checklists.
How Docpolish supports clinical document confidentiality compliance
Handling clinical documents securely during editing and review is a compliance obligation that many organisations overlook until a breach occurs.

Docpolish is built specifically for regulated industries where patient data privacy laws and health document security regulations govern every document interaction. Its client-side PII detection and anonymisation process means that sensitive PHI never leaves the user’s browser before being processed. After professional polishing, the original data is restored in the final output. Every document processed through Docpolish receives a trust identifier, creating an audit trail that supports HIPAA compliance guidelines and demonstrates due diligence to regulators. For compliance officers managing clinical document workflows, explore how Docpolish works to protect sensitive information at every stage of the document lifecycle.
FAQ
What are clinical document confidentiality rules?
Clinical document confidentiality rules are the legal standards governing how healthcare organisations protect, use, and disclose patient health information. In the US, the primary frameworks are the HIPAA Privacy Rule, the HIPAA Security Rule, and 42 CFR Part 2 for substance use disorder records.
How does 42 CFR Part 2 differ from HIPAA?
42 CFR Part 2 applies exclusively to federally assisted SUD treatment programmes and imposes stricter consent requirements than HIPAA. Unlike HIPAA, Part 2 prohibits the use of SUD records in legal proceedings against patients without specific written consent or a qualifying court order.
What is the HIPAA breach notification deadline?
Covered entities must notify affected individuals and the HHS Office for Civil Rights within 60 days of discovering a breach of unsecured PHI. Breaches affecting more than 500 residents of a state or jurisdiction also require media notification within the same timeframe.
What changed in the 2026 Part 2 final rule?
The 2026 Part 2 final rule introduced a single-consent provision allowing patients to authorise future uses and redisclosures by HIPAA-covered entities for treatment, payment, and operations in one consent form. The rule’s strict prohibitions on use in legal proceedings remain unchanged.
What technical safeguards are required for electronic clinical documents?
The HIPAA Security Rule requires encryption, unique user authentication, audit controls, and automatic logoff for systems holding e-PHI. The 2026 CMS standards additionally mandate secure electronic signatures and authenticated document exchange for health care claims attachments.